- Folded Ear in Newborns: Treatment Options - April 11, 2018
- Newborn Ear Deformity: What Can Be Done? - April 11, 2018
- Ear Molding: An Overview - November 2, 2017
- Otoplasty for Protruding Ears - September 26, 2017
- Basal Cell Carcinoma: Facial Reconstruction Timing - September 26, 2017
- Clinical Considerations of Mohs Reconstruction of Cheek Defect - September 26, 2017
- Basal Cell Carcinoma: Nasal Bridge Reconstruction - September 26, 2017
- Skin Cancers Involving the Eyebrow: Clinical Considerations - October 3, 2016
- Treatment of Multiple Skin Cancer Lesions - June 1, 2016
- Skin Cancer: Nasal Reconstruction and Scar Management - June 1, 2016
- India Medical Mission 2018 - November 1, 2018
- Sleep Disorders: Sleep Apnea and Upper Stimulation Therapy - August 25, 2015
- The Naked Vocalist Podcast Featuring Dr. Reena Gupta - May 27, 2015
- New Therapy for Sleep Apnea – First Sleep Pacemaker placed in California at Osborne Head and Neck Institute. - December 12, 2014
- Boxer’s Ear: Can your ear explode? - December 12, 2014
- Nose Picking (Rhinotillexis) and Septal Perforations: Why I should stop picking my nose…? - November 24, 2014
- Deviated Septum and Septal Perforation - July 28, 2014
- Hereditary Hemorrhagic Telangiectasia: Nasal Septal Perforation Repair - June 25, 2014
- Dr. Mantle recognized at the Beverly Hills Medical Science Academy Awards - May 8, 2014
- Commonly Misdiagnosed Pathologies: Arteriovenous Malformations - April 9, 2014
I had a small bump on my nose that my dermatologist said was basal cell cancer. I had it resected and now I have a huge hole in my nose. I need my face to look its best for work and would prefer to have the best result possible. What should I do?

Figure 1: Defect involving the left nasal ala
Case Study
A patient in his sixties noticed a small bump along the left tip of his nose. When he saw his primary care physician he was referred to a dermatologist. A shave biopsy of the lesion was performed and found to be positive for basal cell carcinoma, the most common form of skin cancer. The patient was referred to a Mohs surgeon for resection of the lesion. Arrangements were made for the patient to follow up with Dr. Zandifar following the resection to have the ensuing defect reconstructed. The defect involved the region of the nose referred to as the nasal ala. He underwent a composite graft reconstruction of the nose. There was no need for a large forehead or cheek graft and 3 months later the patient is very happy with the results and is able to breathe through his nose with no difficulty.
Discussion
Defects of the nasal ala are difficult to reconstruct for several reasons. One reason is that the natural curvature of the nose, especially the transition from the outside to the inside of the nostril, is very hard to re-create. Secondly, scarring in the nasal region can cause disfigurement and pulling of the ala. Lastly, alteration to the shape of the ala can change airflow through the nose and in some cases, make it difficult or uncomfortable to breathe.
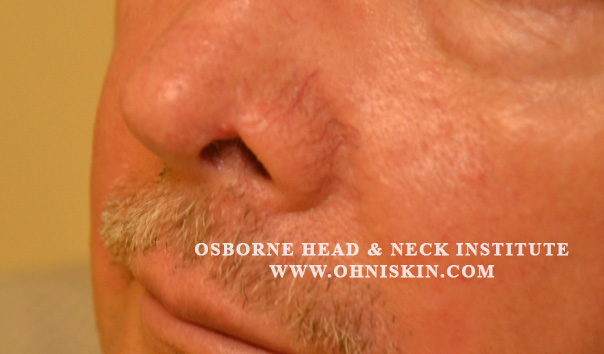 Figure 2: Three months after reconstruction by Dr. Hootan Zandifar
Figure 2: Three months after reconstruction by Dr. Hootan Zandifar
Reconstruction of the nasal ala requires meticulous planning and customization of a procedure suitable to the patient’s specific anatomy. Many times a graft of skin with extra support is needed to reconstruct the alar region of the nose. These grafts are usually harvested from the ear and carry cartilage with them to prevent collapse of the nasal ala. Conversely, other procedures can involve the transfer of a large skin flap from the cheek or forehead.
Nasal reconstruction should ideally be performed by a Facial Plastic and Reconstruction Surgeon with extensive experience. These surgeons are familiar with the nuances of the nasal architecture and can avoid common pitfalls seen when outdated or inappropriate procedures are used.
The physicians of the Osborne Head and Neck Institute are board certified in both otolaryngology and facial plastics and reconstructive surgery. This unique combination of specialties allows the physician to address the functional as well as cosmetic aspects of nasal reconstruction.
To learn more about Dr. Hootan Zandifar or nasal reconstruction following skin cancer resection, please visit: www.ohni.org.



{kind=link}