- Parotidectomy: Deep vs Superficial Lobe - September 26, 2016
- India Medical Mission 2018 - November 1, 2018
- Sleep Disorders: Sleep Apnea and Upper Stimulation Therapy - August 25, 2015
- The Naked Vocalist Podcast Featuring Dr. Reena Gupta - May 27, 2015
- New Therapy for Sleep Apnea – First Sleep Pacemaker placed in California at Osborne Head and Neck Institute. - December 12, 2014
- Boxer’s Ear: Can your ear explode? - December 12, 2014
- Nose Picking (Rhinotillexis) and Septal Perforations: Why I should stop picking my nose…? - November 24, 2014
- Deviated Septum and Septal Perforation - July 28, 2014
- Hereditary Hemorrhagic Telangiectasia: Nasal Septal Perforation Repair - June 25, 2014
- Dr. Mantle recognized at the Beverly Hills Medical Science Academy Awards - May 8, 2014
- Commonly Misdiagnosed Pathologies: Arteriovenous Malformations - April 9, 2014
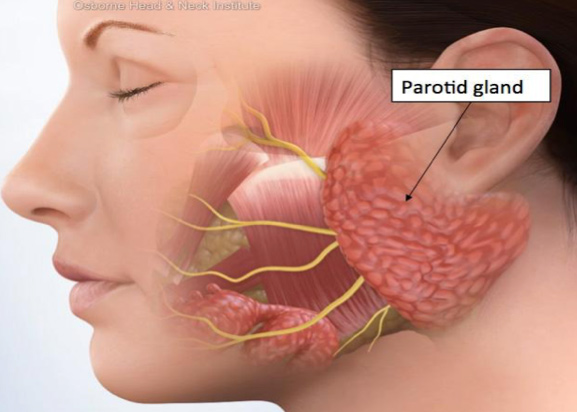
What is the Parotid Gland?
The parotid gland is a bilateral salivary gland, located on either sides of the mouth and in front of both ears, anatomically it is shaped like an upside-down triangle and lies in front of and below the opening of the ear canal. The facial nerve, which runs through the parotid gland, anatomically divides the parotid gland into two lobes- the deep and superficial lobes.
The parotid gland’s primary function is to produce saliva, a watery solution that contains a large concentration of macromolecules and electrolytes, this solution lubricates and aids in the breakdown of food.
The Parotid Gland:
- Looks like an upside down triangle next to your ear
- Produces saliva that helps breaks down food
- Divided by the facial nerve into two lobes
- Superficial lobe – above the facial nerve
- Deep lobe- under the facial nerve
Deep Lobe Parotidectomy
Tumors that are located right under the facial nerve are called deep lobe parotid tumors, if you happen to have this rare type of tumor please consult a head and neck surgeon that has had extensive experience with these particular type of tumors. Due to the rarity of these tumors, a typical head and neck surgeons only perform 0-4 of these procedures a year.
“Deep lobe” parotid tumors are particularly complex and complicated to remove. Typically, these tumors venture beyond the confines of the parotid capsule, wrapping around important structures beyond the facial nerve including: the carotid artery, jugular vein, lingual nerve, vagus nerve, and glossopharyngeal nerve. These structures are all all vital to the proper functioning of the sensory and motor control of the face.
The challenge of removing a deep lobe tumor while preserving the parotid gland is incredible, although every case is different there are some procedures that dramatically improve the ability to preserve physical and cosmetic functions.
Procedures include:
- Contrast sialography
- Sialoscopy
- Parotid Sialendoscopy
- Diagnostic imaging: Computed Tomography (CT) & Magnetic Resonance Imaging (MRI)
- Conducted to help locate the tumor and address complications
- Identifying and preserving vital structures, i.e facial nerves
- Fine needle aspiration
- Helping surgeon to physically diagnose the tumor
Technical Difficulties
Unintentional injury to the facial nerve is a present risk. This risk must be explicitly discussed with every patient undergoing parotid surgery. Even with ostensibly perfect technique, facial nerve injury can occur for unknown reasons, for this very reason it is key to find an experienced head and neck surgeon with extensive anatomical knowledge of the parotid gland.
Possible damage to the facial nerves?
The facial nerve runs directly through the center of the parotid gland. The facial nerve is responsible for all facial functions, damage to this nerve will result in weakness of the muscles on one side of the face. Most nerve damage is a result of bruising of the facial nerve. If this type of nerve damage does occur, then it is usually temporary and it takes only a few months to recover.
- Facial Nerve: nerve that makes your face work, ie smiling & frowning
- Damage is usually in bruising of the nerve
- Takes a few months to heal
- Usually temporary
How is damage to the facial nerves prevented?
Head and neck surgeons prioritize the identification and dissection of the facial nerve for the means of preserving it. The basic principle to the approach is to avoid stimulation of the nerve. Once the facial nerve is identified, specific tools are used during surgery to prevent inadvertent stimulation of the facial nerve. This also typically includes avoidance of electrocauterization techniques.
Surgical Prevention-key points:
- Identify the facial nerve
- Avoid inadvertant stimulation of the facial nerve, ie electrocauterization
Superficial Lobe Parotidectomy
If the tumor is located on top of the facial nerve it is called a superficial lobe parotid tumor. A skilled head and neck surgeon is needed for both a deep and superficial lobe parotidectomy due to the close proximity of the facial nerve to the surgical site.
Superficial lobe tumors are the most noticeable, they often form a visible lump that is called a neoplasm or tumor. This cancerous lump has a risk of metastasizing, or spreading to other sections of the face and body.
Diagnostic tools used in the evaluation of deep lobe parotid tumors are similar to those used in superficial lobe parotid tumors.
Diagnostic and Imaging evaluation tools include:
- Diagnostic imaging, ie Computed Tomography (CT) & Magnetic Resonance Imaging (MRI)scans
- Fine Needle Aspiration
- Parotid Sialendoscopy
- Contrast sialography
Technical Difficulties
Many of the difficulties shared in a deep lobe parotid tumor are still present in a superficial lobe parotid tumor, this is again due to the presence of the facial nerve. Most of the underlying difficulties in a superficial parotidectomy involve avoiding indirect harm to the facial nerve and a safe removal of the tumor, without having to remove much of the parotid gland. A safe removal includes, making sure that the entire tumor is removed; in order to avoid any “spillage” of malignant cancer cells.
General Surgical Procedures and Precautions include:
- Avoiding facial nerve injury
- Removal of the tumor with surrounding parotid tissue
- Minimizing capsular dissection
- Avoiding tumor spillage
Possible Post-Operative Adverse Effects
Possible complications involved with a deep or superficial lobe parotidectomy include:
- Frey’s Syndrome
- Redness and sweating on the cheek area (surgical site)
- Typically correctable with medication [Neurotoxin]
- Numbness
- Facial Asymmetry
- Necrosis
- Death of (skin) cells due to loss of blood supply
- Tumor Reappearance
- Paralysis of the face
- Result of injury or purposeful resection (removal) of the facial nerve.
- If injury or purposeful resection is to occur the surgeon will attempt to reconstruct the nerve or graft a nerve to the injured/severed site
- Result of injury or purposeful resection (removal) of the facial nerve.
- Redness and sweating on the cheek area (surgical site)
All parotidectomy cases should be evaluated and treated by a qualified and experienced head and neck surgeon. These physicians are specialized in the diagnosis and treatment of head and neck cancers including salivary gland tumors.
To learn more about deep and superficial lobe parotidectomy, please visit: www.parotid.net.

{kind=link}