
- Congenital Anotia and Its Repair - January 6, 2020
- Folded Ear in Newborns: Treatment Options - April 11, 2018
- Newborn Ear Deformity: What Can Be Done? - April 11, 2018
- Ear Molding: An Overview - November 2, 2017
- Otoplasty for Protruding Ears - September 26, 2017
- Basal Cell Carcinoma: Facial Reconstruction Timing - September 26, 2017
- Clinical Considerations of Mohs Reconstruction of Cheek Defect - September 26, 2017
- Basal Cell Carcinoma: Nasal Bridge Reconstruction - September 26, 2017
- Skin Cancers Involving the Eyebrow: Clinical Considerations - October 3, 2016
- Treatment of Multiple Skin Cancer Lesions - June 1, 2016
- Skin Cancer: Nasal Reconstruction and Scar Management - June 1, 2016
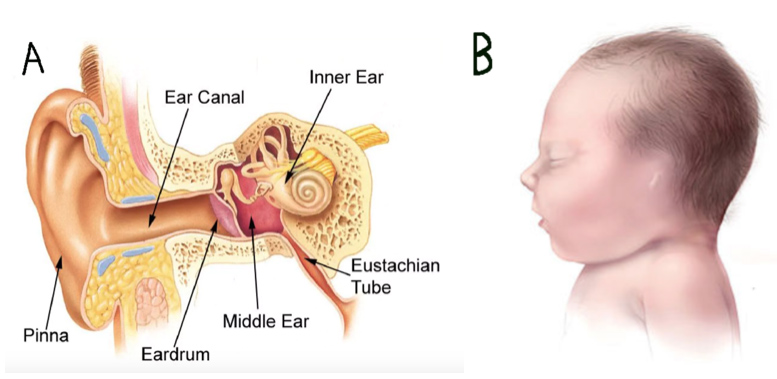
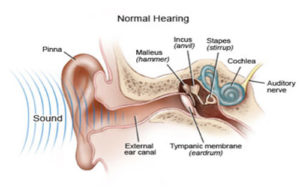
The human ear is a vital structure for both hearing and facial symmetry. It is comprised of three regions: the external ear, the middle ear, and the inner ear. The external ear consists of the pinna (externally visible), the external auditory canal (ear canal), and the tympanic membrane (eardrum). The pinna and external auditory canal are responsible for guiding sound waves from the outer world to the tympanic membrane (ear drum). The middle ear starts at the tympanic membrane and houses the three bones that transmit sound vibrations from the external ear to the inner ear as well as the eustachian tube, which extends to the nasopharynx. The inner ear refers to the cochlea, the auditory nerve, and the structures of balance. Structures in the inner ear convert the sound into signals which are sent to the brain’s auditory cortex by way of the auditory nerve and then to the brain.
The external ear’s reception of sound, the middle ear’s transmission of sound, and the inner ear’s conversion of sound come together to form normal cohesive hearing. Malformation, deformity, or injury of any of the regions results in impaired hearing.
What is Congenital Anotia?
Congenital anotia is a birth defect that refers to the absence of one (most common, 79-93%) or both pinna(e). This is often accompanied by a more narrow or even nonexistent ear canal. Regardless of the functionality of the middle and inner ears, the patient experiences hearing loss in that region along with a cosmetic deformity. A CT scan can help determine the extent of the deformity. Possible variants include:
- the presence/absence of the external auditory canal
- the presence/absence of the middle ear bones
- the presence/absence of the cochlea.
Reconstructive surgery to restore hearing and aid transition to school and avoid social stigma would be performed between the ages of 5 and 10 years old. At this juncture, the unaffected ear, if present, will have reached 85-95% of its adult size. The patient will have enough rib cartilage for reconstruction, if this is what is chosen, and the patient will likely possess a sufficient level of emotional maturity.
What is the method of reconstruction3?
One of the most common and effective procedures for ear reconstruction is the Brent method. It requires four surgeries to construct a functional and aesthetically appealing external ear made entirely from the patient’s own tissue. Each surgery should be performed approximately two to three months apart to ensure proper healing.
Stages of Brent Method Reconstruction:
- Rib Cartilage Graft (Harvesting and Placement)
Ear reconstruction begins with the creation of an ear template from the unaffected ear if available. The template is used to approximate the amount of rib cartilage needed for reconstruction. The surgeon then harvests the rib cartilage and molds it into the shape of an ear. The cartilage graft is inserted under the scalp in the ear’s natural position.
- Lobule Transposition
Lobule transposition refers to the creation of the ear lobe.
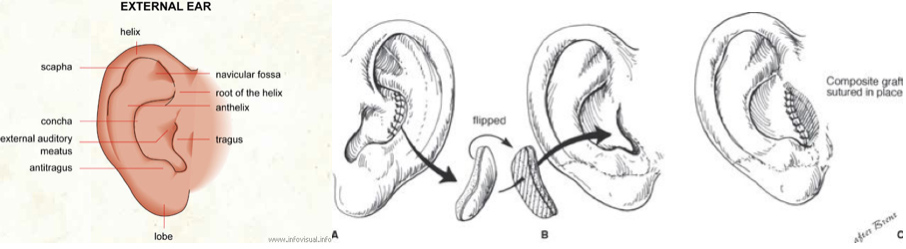
- Tragus Construction
The surgeon creates the tragus from a composite graft of the unaffected ear.
- Separating the Ear
In the fourth and final surgery, the surgeon elevates the ear structures away from the scalp flap and covers the posterior section with a skin graft. A sulcus (where the ear meets the skull) is now defined and the ear separates from the cranium.
Can hearing be restored?
Fortunately, the external and middle ear have different embryological origins than the inner ear; therefore, many anotia patients retain the neurological potential to hear despite the deformity. An audiogram, Weber test, and Rinne test must be performed to determine whether the patient suffers from conductive hearing loss or sensorineural hearing loss. A CT scan is also essential in determining the status of the ear canal and middle ear structures. The ear surgeon uses several criteria to determine if the ear canal and middle ear can be reconstructed, or if bone conduction hearing implants should be utilized. The surgery to open the ear canal is called a canalplasty. The surgery to reconstruct the middle ear is called a tympanoplasty. In appropriately selected patients, this surgery can successfully restore the natural hearing mechanism of the ear without the use of a hearing device.
A Bone Anchored Hearing Aid (BAHA) can be either worn or implanted to restore hearing as long as the patient has a functional cochlea. A BAHA may be worn as a soft headband when the patient is under 5 years old; at the appropriate age, a titanium implant can be coupled to a sound processor to allow even better sound conduction. A BAHA implant does not require any surgery on the ear canal or middle ear, and vital structures such as the facial nerve or inner ear are safe from harm. The implant is placed behind the ear through a small incision on the scalp, and is tightened a few millimeters into the skull. The sound travels through the implant and vibrates the cranial bones to the cochlea instead of through the external and middle ear.
Key Points:
- Congenital Anotia is the absence of the external ear, often accompanied by a narrow or absent ear canal
- A CT scan is necessary to discover what anatomical elements are absent or malformed along with the best surgical course of action
- The most beneficial time for ear reconstruction is between the ages of 5 and 10
- The Brent method is a four surgery process of ear reconstruction that utilizes the patient’s own cartilage and skin
- An audiogram, Weber test, and Rinne test must be performed to determine the type of hearing loss one suffers from
- BAHA and canalplasty are two ways to restore conductive hearing loss in patients with anotia.

{kind=link}