- Question: How do the ingredients in e-cigarettes and vaporizers affect respiratory health? - August 16, 2019
- Bad Technique and Vocal Injury - January 9, 2019
- Is Edible Marijuana Dangerous for the Voice? Myths Dispelled - December 18, 2018
- Surprise! You have a hemorrhage - January 31, 2018
- Graves’ Disease: Treatment Overview - September 25, 2017
- Adele and the Stigma of Vocal Injury - July 11, 2017
- Vocal Curbside Consult: How does the thyroid affect the voice? - May 16, 2017
- Vocal Curbside Consult: How do hormones affect the voice? - May 3, 2017
- Vocal Curbside Consult: How do emotion and stress affect the voice? - April 17, 2017
- Vocal Curbside Consult: Vocal Recovery After Illness - April 7, 2017
The patient is a 32 year old singer who presented with significant worsening of her voice over a 3 month period. She is typically in meetings for most of the day where she engages in significant and loud voice use. In the evenings, following her workday, she is at rehearsals or in the studio. The patient is now experiencing discomfort associated with voice use and difficulty projecting her voice without significant effort. Her vocal range is also decreased, but she is able to push to access her full voice. She is a non-smoker and rarely drinks alcohol. She is not taking any prescription or non-prescription medications or supplements.
Her initial voice recording is here:
Initial videostroboscopy is presented here:
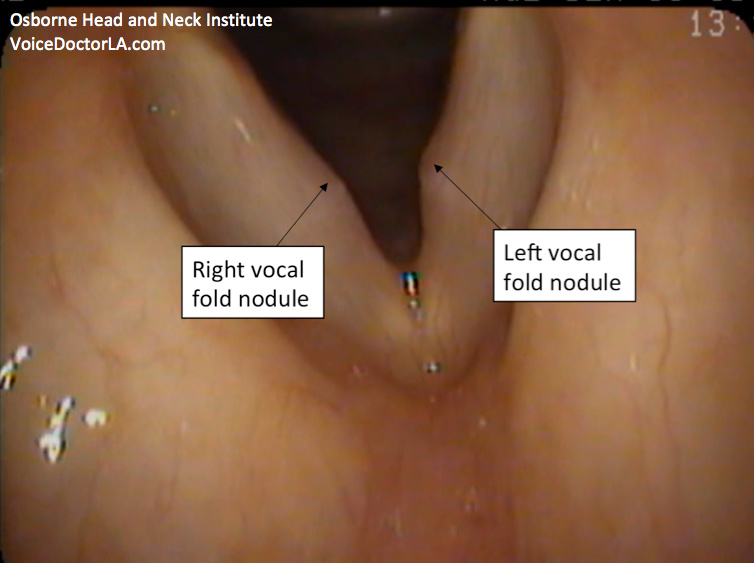
Because of the patient’s severe gag reflex, this exam was performed with a flexible distal chip laryngoscope (through the nose) in lieu of high definition videostroboscopy (through the mouth). The use of flexible laryngoscopy typically results in a lower resolution image, as is seen here. More on the differences in these imaging technologies may be found here. Note that the referenced article contrasts traditional fiberoptic laryngoscopy with rigid stroboscopy. In our patient’s case, superior distal chip technology (digital), not fiberoptic, was used.
There is a large nodule on her left vocal fold and a smaller one on her right that are severely affecting vibration. Strobe light is used and she attempts to phonate but no wave is produced due to the severity of the nodules. At the end of the video, I switch back to straight (halogen) light and zoom in further to show the lesions better.
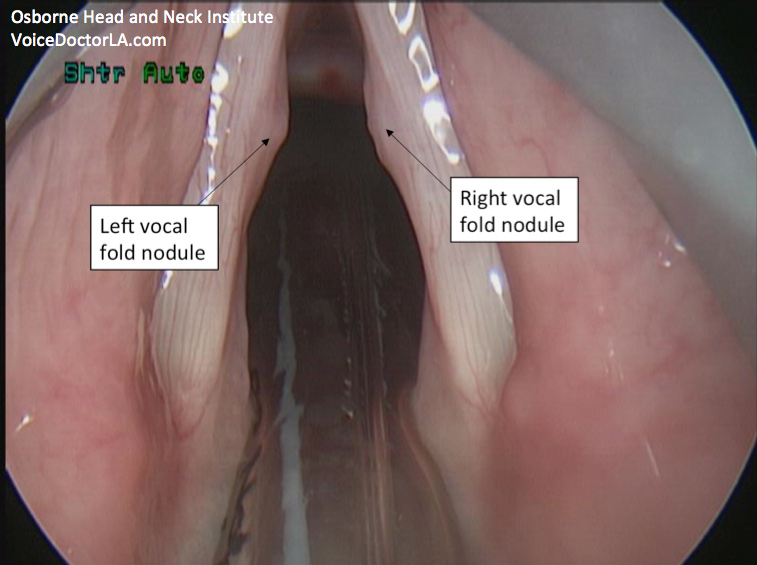
A trial of voice therapy was suggested and the patient was compliant. However, she did not note any improvement. A decision was therefore made to perform conservative surgery. Intraoperatively, this is the image of her vocal folds. Note that operative views are rotated 180 degrees, so that right is right and left is left (unlike office laryngoscopy which is like a mirror – left is right and right is left).
Careful operative excision and adjunctive injections were performed. She was placed on strict voice rest and followed up for therapy after surgery.
At two weeks, repeat stroboscopy was performed and a normal mucosal wave is observed. Her vocal quality is the best it has been in years and she feels that speaking is effortless. Her audio and video from after surgery are presented here. The continued mild raspiness audible in her voice is due to speaking technique, as evidenced by the fact that she is clear at times. Continued vocal therapy will be needed to resolve this.
Critical take-home points:
- Sometimes nodules require surgery. This is rare; anyone who has worked with me knows that I advocate therapy almost exclusively for nodule treatment. Experience and expertise are required to be able to determine which patients will benefit from surgery and which will not. When good selection criteria are not used, outcomes are poor. This case highlights that even when surgery is performed for nodules the outcome can be excellent. However, this requires optimal vocal therapy, appropriate diagnosis, careful assessment for surgical candidacy, and skilled surgery. Patients fail when even one of these 4 things are not in place.
- It is critical to see the vocal folds optimally for diagnosis. Those familiar with the Voice Case of the Week have gotten used to rigid stroboscopy images and are probably frowning at the lower-resolution distal chip pictures in this case. Imagine having even lower resolution fiberoptic technology (which is what most ENTs have in their offices)! This is why misdiagnosis occurs.
- To re-emphasize this point, look at the difference in the resolution of the operative view. The nodules are obvious in that picture. This is the highest resolution available. See how much even a distal chip flexible laryngoscope misses? Again, a fiberoptic flexible laryngoscope is no longer acceptable to visualize vocal folds. You will know you’ve had this inadequate exam if it looked like the example in this article, demonstrated for teaching purposes by my colleague, Dr. Ryan Osborne.
- Nodules are not a death sentence for a singer. Indeed, most accurate diagnoses are not. However, all pathology has gotten a bad rap because of ENTs using poor technology and misdiagnosing singer’s real problems. The fear singers have about seeing a doctor when they have problems comes from horror stories that I believe started with misdiagnosis and ended with inappropriate treatment. The best advice is for singers to be their own advocates, demanding a fellowship-trained laryngologist with distal chip laryngoscopy and rigid stroboscopy as well as excellent surgical results.
To learn more about Dr. Reena Gupta or vocal nodule evaluation and treatment, please visit www.voicedoctorla.com.



{kind=link}