- Question: How do the ingredients in e-cigarettes and vaporizers affect respiratory health? - August 16, 2019
- Bad Technique and Vocal Injury - January 9, 2019
- Is Edible Marijuana Dangerous for the Voice? Myths Dispelled - December 18, 2018
- Surprise! You have a hemorrhage - January 31, 2018
- Graves’ Disease: Treatment Overview - September 25, 2017
- Adele and the Stigma of Vocal Injury - July 11, 2017
- Vocal Curbside Consult: How does the thyroid affect the voice? - May 16, 2017
- Vocal Curbside Consult: How do hormones affect the voice? - May 3, 2017
- Vocal Curbside Consult: How do emotion and stress affect the voice? - April 17, 2017
- Vocal Curbside Consult: Vocal Recovery After Illness - April 7, 2017
The patient is a 40 year old female who has had significant vocal symptoms for several months. She has noted a decrease in her vocal range and increased effort during phonation. She previously saw a laryngologist, who diagnosed her with a vocal polyp. She was referred for voice therapy, but based on her failure to improve, went back to her surgeon for a surgical consultation. She did not feel comfortable with the recommendation and sought a second opinion here at the Osborne Head and Neck Institute.
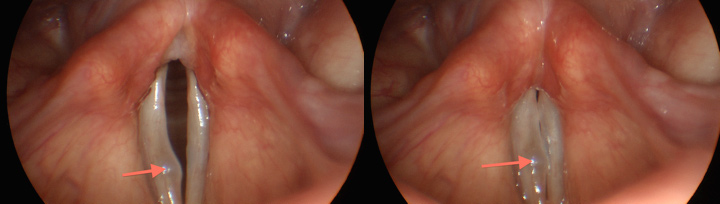
Stroboscopy was performed:
This is an unusual case in that the patient does not have a true vocal polyp. Instead, she has polypoid corditis. Polypoid corditis occurs when the superficial lamina propria (SLP) becomes more gelatinous. This crucial vibrating layer normally has greater viscosity than, for example, water, but it is not very firm. In some people, often smokers, the SLP becomes more gelatinous and firm, preventing normal vibration.
The distinction between a vocal polyp and polypoid corditis is a critical one to make. This is because the surgical plan is completely different and, most importantly, the prognosis is different. A vocal polyp tends to be a very straightforward surgery, with excellent results expected. Polypoid corditis, however, is a much more involved surgery. It involves an incision into the vocal fold and excavation of polypoid material while taking care to preserve enough lamina propria to permit vibration.
It is critical to inform the patient appropriately prior to undergoing surgery, because the risk profile is so different between vocal polyps and polypoid corditis. Indeed, the polypoid corditis patient may elect to not proceed with surgery, as the vocal outcome is less predictable. All said, it is still likely to be a successful surgical intervention. However, the dissatisfied patient often results from unreasonable expectations. Misdiagnosis is the surest way to guarantee this outcome.
Perhaps most troubling is that this patient was knowledgeable enough to seek care from a specialized provider, a laryngologist. There is no good explanation as to why a physician who is theoretically trained well enough to provide better care than this did not do so. This may be where a good relationship between physician and vocal coach is most vital. By developing this relationship, a vocal coach can provide a referral to a skilled laryngologist that is more likely to yield an accurate diagnosis and in turn improve surgical outcome and patient satisfaction.
To learn more about Dr. Reena Gupta or polypoid corditis, please visit www.voicedoctorla.com.



{kind=link}